| The main diseases |
| Contents |
|
The pathway taken by air when we breathe is called the respiratory tract or the air way, and the section of this pathway from the bronchus to the alveoli is the lung. Cancers that arise anywhere along this section are known as lung cancers. At present, the one cause of lung cancer that is clearly known is smoking. Lung cancer is the cancer with the highest mortality in Japan. The treatment method for lung cancer is generally decided according to the stage of the cancer, which classify the progression of the disease. In addition, the method used for treatment is carefully selected on the basis of the characteristics of the cancer, the patient’s age, prior diseases, the presence of any complications, the functioning of the internal organs, and the patient’s general health. The treatments available for lung cancer include surgery, radiation therapy, chemotherapy using anticancer drugs, immunotherapy, and treatment for pain or other distress that aims to relieve symptoms (palliative care). Surgery is mainly carried out for the stages I or stage II diseases.
Figure 5: Statistics on lung cancer in Japan
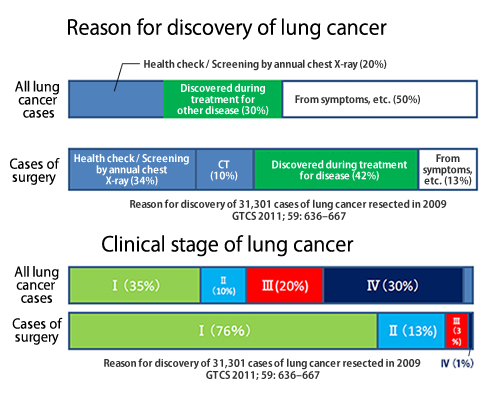
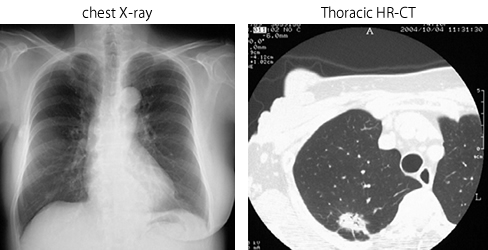
Figure 6: Small-sized lung cancer, which has recently become more common
The standard operative procedure is removal of the lobe of the lung (lung lobectomy) where the cancer is present, together with complete removal of the lymph nodes (lymph node dissection). With stage I and stage II lung cancers, the technique of making a small incision and inserting a video camera called a thoracoscope has become common. The images from inside the chest obtained from this device are viewed on a monitor, and lung resection is performed using a range of devices, such as an automatic suture instrument (stapler).
Figure 7: Thoracoscopic lobectomy for lung cancer

The thoracoscope between the two surgeons displays an image of the inside of the chest on the monitor screen, and the surgeons are working together to expose the blood vessels in order to remove the lung. The operative field is magnified, enabling the surgeons to accurately grip the thin membrane that needs to be peeled off. In an operation carried out with direct vision, there is a clear division of duties between the surgeon and the assistant, but when the thoracoscope is used, it is as if there were two surgeons and four hands, which reduces the time required for the operation.
In the case of stage III lung cancer, such as superior sulcus tumor, in which the cancer invades the chest wall with a pain in the shoulder and chest wall, chemotherapy and radiation therapy are first carried out. A standard thoracotomy is then carried out by making an incision between the ribs, and the surgeon directly observes the operating field and removes a lung and an area of chest wall en bloc.
Figure 8: Superior sulcus tumor
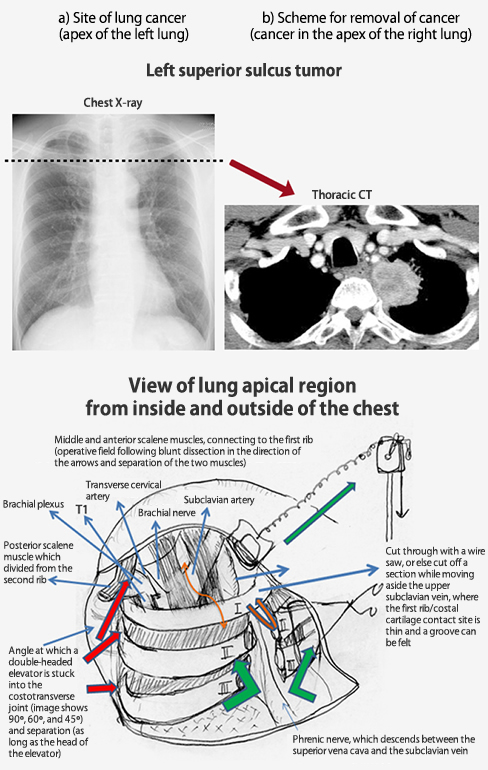
This type of surgery is called “extended surgery,” because rather than only the lung, the lung and the chest wall contiguous with the lung cancer are removed en bloc.
The space between the lungs and the chest (from the chest wall to the diaphragm), in which the lungs are contained, is called the thoracic cavity. This space, just a few hundredths of a millimeter thick, contains a few cubic centimeters of fluid that acts as a lubricant when the lungs expand and contract. This allows the lungs and the chest to move smoothly against each other. Pneumothorax is a condition in which air leaks from a lung and collects in the thoracic cavity. When this happens, the air that has leaked into the thoracic cavity pushes against the lung, making it smaller.
Figure 9: Right spontaneous pneumothorax in a young man with a thin physique
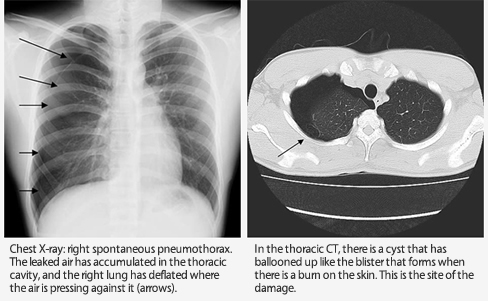
The problem with pneumothorax is that relapse can occur. Surgery is needed to remove the bulla (balloon-like condition on the surface of the lung) causing the pneumothorax. In many cases, thoracoscopic surgery is selected.
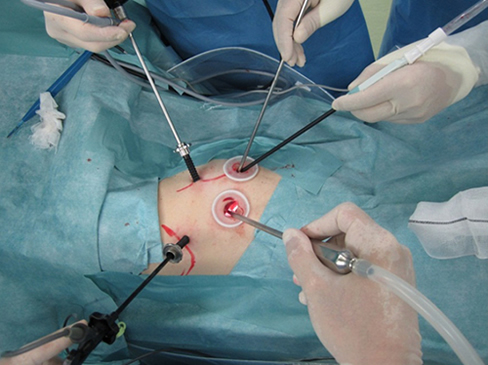
Figure 10: Thoracoscopic surgery being carried out (photos courtesy of Dr. Mun Mingyon of the Department of Thoracic Surgery, Cancer Institute Hospital)
1. The surgeons look at the monitor while performing surgery

2. Surgical instruments are inserted through several small incisions made in the chest.
The lung is one of the organs to which malignant tumors readily migrate, and tumors that have migrated from other organs to the lungs in the bloodstream or lymphatic flow are known as metastatic lung tumors (metastatic lung cancer). Different types of treatment are selected for metastatic lung tumors, depending on the characteristics of the primary lesion (the organ in which the cancer originally developed), and the options include surgical removal. However, the effects of removal of a lung need to be taken fully into consideration, and in most cases of metastatic tumor, just the cancerous part is removed. The table shows the primary lesions from the results of the 2010 academic survey carried out by the JATS.
| Main primary lesion | No. of patients |
|---|---|
| Colon | 3,352 |
| Kidney | 543 |
| Cervicofacial region | 436 |
| Breast | 397 |
| Lung | 351 |
| Uterus | 300 |
| Liver/pancreas | 289 |
| Soft tissue | 270 |
| Bone | 121 |
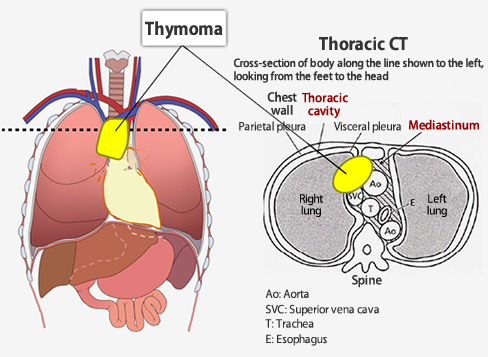
The thymus is located behind the sternum, above and to the front of the heart (this region is called the anterior mediastinum). This organ is responsible for maturation of white blood cells called T-lymphocytes, which are related to immunity. When adulthood is reached, the work of the thymus is finished, and it degenerates into fatty tissue. A thymoma is a tumor that develops in the degenerated thymus of adults. The speed of multiplication of the tumor cells is relatively slow, and the neoplastic cells do not commonly spread outside the thymus. However, if thymoma develops, it sometimes extends to the neighboring organs including lungs, major vessels, pericardium, heart, or thoracic cavity. The most common treatment for thymoma is surgery, which is performed to completely remove the thymus and the surrounding tissues to which the tumor is suspected to have spread. Normally, this is done by opening up the skin in the center of the chest (this is called median sternotomy). Also, thoracotomy (a surgical incision of 5–10 cm) and thoracoscopic surgery are generally used for small tumors.
Figure 11: The site of thymoma
The organs inside the chest and the abdomen are covered by membranes. In the chest, the lungs are covered by the pleura and the heart by the pericardium, while in the abdomen, the stomach, liver, and other organs are covered by the peritoneum. These thin membranes are made up of mesothelial cells arranged side-by-side. Cancer that develops from these mesothelial cells is called mesothelioma. Pleural mesothelioma, pericardial mesothelioma, or peritoneal mesothelioma can arise depending on the site from which the cancer develops. Mesothelioma means that it is a malignant tumor. In the case of pleural mesothelioma, it may be necessary to perform a major operation to remove all of one lung, the outer pleura (the parietal pleura), and the diaphragm all at once. This is called pleuropneumonectomy. There is also a procedure in which the outer pleura is removed, and the inner pleura, which has thickened due to the tumor, is taken away. In this case, the lung is left in place. Chemotherapy with anticancer drugs may be carried out first, and radiation therapy may also be carried out to prevent relapse after surgery.
Figure 12: The lesions of mesothelioma

Observation made by inserting a videoscope into the thoracic cavity. The things that appear to be stuck to the diaphragm, visible as a raised area in the center, and the pleura, which covers the chest wall at the top of the photograph, are pleural mesothelioma. Pleuropneumonectomy was performed following chemotherapy with anticancer drugs, after which radiation therapy was carried out on the right lung.
Pyothorax is an accumulation of suppurative fluid in the thoracic cavity, which may be caused by systemic blood poisoning, external trauma, or pneumonia. Bacterial pyothorax is the most commonly encountered type, and it is known as acute pyothorax if it is within a few weeks of onset. If a few months have passed since onset, and a multilayered membrane has formed on the surface of the lung, so that the lung is unable to inflate to its normal shape, the condition is called chronic pyothorax. The general rule for pyothorax treatment is to provide thorough treatment during the acute phase in order to prevent a transition to chronic pyothorax. The treatment methods are antibacterial drugs and drainage of the thoracic cavity, but if a membrane of fibrin has formed, a surgical procedure is performed. Fibrin is a protein that causes coagulation of blood. When there is bleeding, thrombin acts on fibrinogen in the plasma to form fibrin, which is insoluble and filamentous. If fibrin has formed, the condition inside the thoracic cavity is checked with a thoracoscope, the accumulated fibrin and contaminated tissue are scraped away, and the area is washed with copious amounts of saline solution. If the pyothorax has become chronic because of delayed detection or intervention, and the lung cannot inflate fully with the above treatments or procedure, the treatment is carried out by selecting fenestration, lung decortication, pleuropulmonary resection, or thoracoplasty according to the condition, in order to remove the pyothorax cavity.
Radical dissection of early stage pyothorax
1970s: Mini-thoracotomy
1990s: Video-assisted |
Figure 13: Left bacterial pyothorax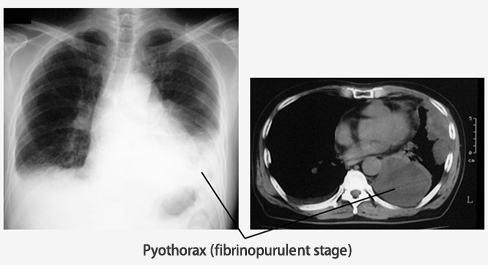
The left lung is flattened by the accumulation of sludgy pleural fluid in the thoracic cavity (pyothorax) as a result of bacterial infection.
© The Japanese Association for Thoracic Surgery. All Rights Reserved.